

Translate this page into:
A PATH LESS LOOKED FOR - MIDDLE MESIAL CANAL : CASE SERIES
Corresponding Author : Dr. Arpit Sikri
This article was originally published by Indira Gandhi Institute of Medical Science and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Knowledge of pulp anatomy of mandibular molar is crucial for endodontic treatment success. There are innumerable causes for endodontic failures but missed canals comes out to be the most common. Each canal contains irregular and hidden regions, which have to be accessed during endodontic therapy. The advent of latest technological advancements in the field of dentistry leads to the identification of the variable root canal anatomy that helped in increasing the success rate. The present case series portrays the successful management of the middle mesial canals with different anatomical configuration in case of mandibular molars.
Keywords
Dental operating microscope
mandibular molar
middle mesial canal
root canal anatomy
root canal system

INTRODUCTION:
Diversification in the root canal system requires thorough knowledge and skill of operator to diagnosis and manage the complex anatomy with accuracy to nullify the failure rate. The mandibular molars are most frequently involved in the root canal treatment, as they are the first tooth to erupt and get more exposure in the oral cavity, hence more prone to caries activity. According to the textbooks, they have two roots (mesial and distal) and three canals (mesiobuccal, mesiolingual and distal), but now a days due to the advent of newer technologies, recent studies have been published to describe different types of root canal variations in case of mandibular molars1 e.g. Radix Entomolaris, Radix Paramolaris (Three roots), Extra Distal Canal, Extra Mesial Canal and C-shaped canal etc.2 Extra mesial root canal is most commonly present between the buccal and lingual canal and known as the Middle Mesial Canal or Mid Mesial canal1. Middle mesial canal (MMC) was first reported by Barker et al in 19743,4,5 as independent third canal in the mesial roots of mandibular molars. After that, Pomeranz et al in 1981 classify the MMC into 3 categories (Figure 1)1,2

- Classification of Middle Mesial Canal
Independent type: the canal originates from a separate orifice and continues independently without interacting with the mesiobuccal or mesiolingual canals all the way to the apex.
Confluent type: the canal fuses and continues with either the mesiobuccal or the mesiolingual canal.
Fin type: the canal is joined by an isthmus with the mesiobuccal or mesiolingual canal along its path.
The incidence of MM canal according to previous studies was found to be 0-15%. With the onset of advanced technology, the incidence increased to 45.85% in the first molars and 53.8% in the second molars.6
Being an Endodontist, the prime intention is to have a sound knowledge of different types of root canal anatomy of all the teeth, proper diagnosis, use of advance technology and techniques to minimize the risk of missed canals and spaces within the root canal system. These missed canals contain microorganisms and their by-products which becomes the major cause of post-operative failure due to persistence periapical inflammation.7
This paper describes the detection and management of middle mesial canal in case of first mandibular molar.
CASE REPORT 1:
A 25 years old patient reported to the Department of Conservative Dentistry and Endodontics with the chief complaint of pain and discomfort in the lower left back tooth region from 2 weeks. On clinical examination, deep occlusal caries was present, tender on percussion and showed negative response when pulp sensibility test8,9 was performed. The preoperative IOPA w.r.t 36 (Figure 2) confirmed deep carious lesion involving pulpal space with PDL space widening. A provisional diagnosis of Necrotic Pulp with apical periodontitis w.r.t 36 was made and planned for root canal therapy.

- Pre-Operative IOPA w.r.t 36
After the administration of local anaesthesia, tooth was isolated using rubber dam. Once the anaesthesia was effective, all the carious lesion was removed using the round bur and access was made with the help of Endo Access Bur. The access opening was enlarged to deroof the pulpal chamber using Endo-Z bur (Safe-ended Bur) (Figure 3), then pulpal floor was properly explored to negotiate the root canal orifice using Dental Loupes (Figure 4). The presence of middle mesial canal was suspected because on visualization of dentinal map, there was gap and depression felt in between the mesiobuccal and mesiolingual orifice. This is one of the clinical tips, that one should look for the presence of an extra mesial root canal. On careful examination of the pulpal floor, we identified five root canal w.r.t 36 (Mesiobuccal, Middle Mesial, Mesiolingual, Distobuccal and Distolingual) (Figure 5) and all the canal were negotiated using 10 no K file. The working length was determined with the help of electronic apex locator (Coltene) and confirmed using radiograph (Figure 6). After achieving the working length, biomechanical preparation was started using Hyflex CM files (Coltene) and copious irrigation was done with 3% Sodium hypochlorite and 17% EDTA. Afterwards, canals were finally rinsed with saline to remove the residual debris and followed by drying using the paper points and calcium hydroxide dressing was placed inside the canals. Patient was recalled after one week and tooth was asymptomatic. Finally, it was obturated with gutta percha cones using sealapex root canal sealer (Figure 7). The patient experienced no postoperative sequelae and an appropriate postendodontic restoration was performed in a subsequent appointment to ensure an adequate coronal seal.

- Endo Z Bur (Safe-ended Bur)

- Dental Loupes

- Clinical photo of Pulpal Floor showing Dentinal Map

- Working Length RVG

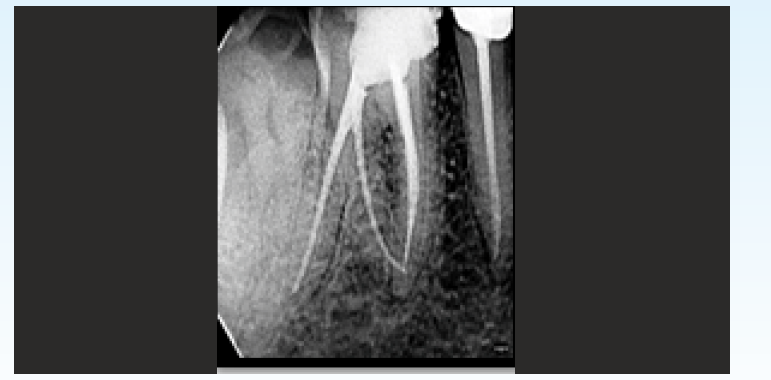
- Master Cone and Obturation Radiograph
CASE REPORT 2:
A 30 years female patient reported to the Department of Conservative Dentistry and Endodontics with unbearable pain w.r.t to right mandibular first molar. On both clinical and radiographical examination (Figure 8), faulty restoration leading to irreversible pulpitis w.r.t 46 was observed. During IOPA reading, 46 showed an extra root known as Radix Entomolaris. The root canal treatment was started after the administration of local anaesthesia. All the faulty restoration was carefully removed and access opening was done by deroofing the pupal chamber so as to gain straight line access to all the root canal orifices. Pulpal floor was meticulously explored under dental loupes to locate the orifices. We found five root canal orifices in this case (Figure 9) (Mesiobuccal, Middle Mesial, Mesiolingual, Distolingual, Distobuccal) as this tooth had extra root also (Radix Entomolaris). The working length was taken with the help of electronic apex locator (Canal Pro, Coltene) and confirmed using digital radiograph (Figure 10). After achieving the working length, biomechanical preparation was started using Hyflex CM files (Coltene) and copious irrigation was done with 3% sodium hypochlorite and 17% EDTA, obturation (Figure 11) was done in the same visit. Patient was recalled after 1 week for the post endodontic restoration and tooth preparation. After 2 days, patient was given the PFM crown (Figure 12) on the particular tooth.

- Pre-Operative Radiograph w.r.t 46

- Clinical Photo of Five Root Canal orifice showing Middle Mesial Canal

- Working Length Radiograph
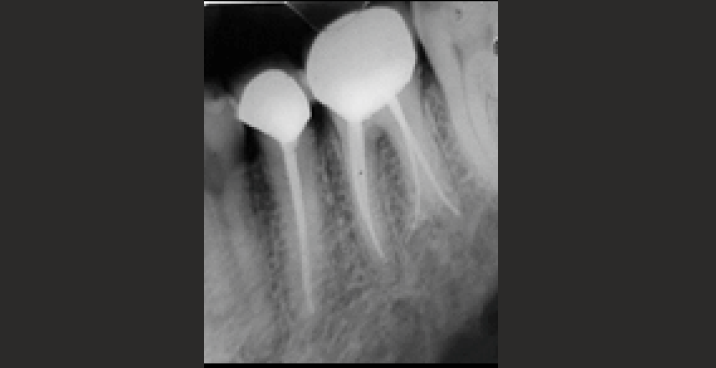
- Obturation
- PFM Crown given w.r.t 46
CASE REPORT 3:
Patient visited to the Department of Conservative Dentistry and Endodontics with chief complaint of pain and sensitivity in right mandibular molar. After taking the RVG of the concerned tooth, deep occlusal caries was seen which was approaching towards the pulp. We decided to perform root canal treatment of 46. After performing the access opening of 46, pulpal floor was explored under Dental Operating microscope and we found an extra canal in mesial root of 46 (Mesiobuccal, Middle Mesial, Mesiolingual) (Figure 13). The glidepath was achieved for all the root canals and working length was taken (Figure 14) w.r.t 46, the biomechanical preparation was done with copious irrigation using 3% sodium hypochlorite. The obturation (Figure 15) and post endodontic restoration was done after one week to achieve a good coronal seal.

- Clinical Photo of Middle Mesial Canal under DOM

- Working Length Determination

- Master Cone and Obturation Radiograph
DISCUSSION:
The prime motto for the successful root canal treatment is to understand the root canal anatomy and its variation, so as to make the entire root canal system bacteria free to reduce the chances of post-operative failures. Middle mesial canals present as a small orifice deep within the isthmus or a developmental groove between the two orifices of the MB and ML canals. In the previous studies, the incidence of MM canal was reported to be 0- 15%.10,11,12,13,14 Azim et al correlated the occurrence of MM canals with age and concluded that younger patients, aged 30-40 years, had a significantly higher incidence of a MM canal. Nosrat et al reported that the incidence of MM canals was 32.1% in patients.5 According to the recent studies, the prevalence comes out to be 10-37.5% in the first molars and 18-60% in the second molars due to appearance of recent technological advancements like magnifying loupes, dental operating microscope, troughing techniques, exploration of dentinal map and CBCT etc.6
Dentinal map also acts as a guide for the negotiation of the root canal orifice, during exploration if there is a gap present between MB and ML orifice, then there are higher chances of presence of Middle Mesial canal. If we suspect the presence of extra canal then troughing technique is quite safe and effective method to locate middle mesial canals in case of mandibular molars, because it requires minimal dentin removal between the MB and ML canals in a mesioapical direction away from the furcal danger zone. Troughing has to be performed very precisely to avoid accidental strip perforation, so it has to regulate under magnification and specialized instruments to be used e.g., small size munce discovery burs and ultrasonic tips. Different authors have suggested that a troughing preparation with a depth ranging between 0.7 and 2.0 mm is adequate.6
With the advent of magnification, clinician efficiency got improved in order to locate and negotiate the MM canal properly. Dental operating microscope or magnifying loupes can be used to visualize the dentinal map present on the pulpal floor but the MM orifice is most probably located below a dentinal projection in the groove between the two main canals (Mesiobuccal and Mesiolingual). The layer of dentin in this groove is lighter in colour than the adjacent dentin. Studies have reported the average length of the groove in mandibular first and second molars to be 1.07-2.81 mm and the average depth to be 1.05 mm and 0.17-7.66 mm15,16. The diameter of a MMC is generally less than that of the two main canals in the mesial root which comes out to be 0.16 mm, three times less than the diameter of the main mesial canal orifices, which is 0.5 mm.4
Other diagnostic aids like dyes, champagne bubble test, ultrasonics, micro openers and trans-illumination aids, irrigators to improve the pulp chamber visibility (Stropko) and observing the chamber for bleeding spots could be used by the clinician as effective measures to locate the additional canal orifices.7
A study conducted by Karabucak et al, which describes about the prevalence of missed canal in endodontically treated teeth with the help of Conebeam Computed Tomography (CBCT), and concluded that the missed canal increases the chances of developing a periapical lesion w.r.t to particular tooth by 4.38 times.17
So, the detailed preoperative and intraoperative assessment of landmarks should be made which will minimize the chances of missed canal, therefore, increasing the success rate of the endodontic therapy.17
Periapical radiograph or RVG can be used for preoperative assessment but keeping in mind the limitations of these techniques like compression of 3-D structures to 2-D imaging, geometric distortions and anatomical superimposition.18 So, we can make good application of the recent radiographic technique like CBCT, which will provide nondestructive 3-D evaluation of the anatomical variations and morphological characteristics of the root canals but the major limitation is the radiation exposure. Moreover, it helps the clinician to visualize the pulpal anatomy in different planes by providing the detailed assessment starting from coronal portion to the apical portion of the root canal.19
CONCLUSION:
When we talk about the mandibular molars, they are the most frequently involved tooth for the endodontic therapy and have variable root canal morphology. C-shaped canal, extra root, extra canal, apical deltas and fins are the most common variations seen in the mandibular molars. Recent studies revealed increased chances of Middle Mesial canal present in the mandibular molars, which was earlier ignored by the clinicians and thereby increased the chances of endodontic failure. While performing the root canal treatment of mandibular molars, we should explore all the possibilities of fluctuations present inside the root canal anatomy. Magnification, CBCT, troughing techniques proved to be the helping hands for the dental surgeon to provide more valuable treatment to the society.
REFERENCES:
- The mid-mesial canal prevalence in mandibular molars of a Saudi population: A cone-beam computed tomography study. The Saudi Dental Journal 2020 Aug:25.
- [CrossRef] [PubMed] [Google Scholar]
- Variable permanent mandibular first molar: Review of literature. J Conser Dent. 2013;16(2):99-110.
- [CrossRef] [PubMed] [Google Scholar]
- Anatomy of Root Canals. III. Permanent Mandibular Molars. Aust Dent J. 1974;19(6):408-13.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and Distribution of the Middle Mesial Canal in Mandibular First Molar Teeth of the Kerman Population: A CBCT Study. International Journal of Dentistry. 2000;31:1-6.
- [CrossRef] [PubMed] [Google Scholar]
- A mandibular second molar with a middle mesial root canal. Clinical Case Reports. 2020;8(6):1015-20.
- [CrossRef] [PubMed] [Google Scholar]
- Advanced methods for identification of middle mesial canal in mandibular molars: an in vitro study. Endodontology. 2016;28(2):92.
- [CrossRef] [Google Scholar]
- Management of middle mesial canal in mandibular second molar. Journal of pharmacy & bioallied sciences. 2012;4(Suppl 2):S161.
- [CrossRef] [PubMed] [Google Scholar]
- Review of pulp sensibility tests. Part I: general information and thermal tests. International endodontic journal. 2010;43(9):738-62.
- [CrossRef] [PubMed] [Google Scholar]
- Review of pulp sensibility tests. Part ??: electric pulp tests and test cavities. International endodontic journal. 2010;43(11):945-58.
- [CrossRef] [PubMed] [Google Scholar]
- Root canal anatomy of the human permanent teeth. Oral surgery, oral medicine, oral pathology. 1984;58(5):589-99.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment considerations of the middle mesial canal of mandibular first and second molars. Journal of endodontics. 1981;7(12):565-8.
- [CrossRef] [PubMed] [Google Scholar]
- Root and canal morphology of Burmese mandibular molars. International endodontic journal. 2001;34(5):359-70.
- [CrossRef] [PubMed] [Google Scholar]
- Unusual root anatomy of mandibular first molars. Journal of endodontics. 1985;11(12):568-72.
- [CrossRef] [PubMed] [Google Scholar]
- Three canals in the mesial root of mandibular first permanent molars: a clinical study. International endodontic journal. 1989;22(1):39-43.
- [CrossRef] [PubMed] [Google Scholar]
- Root canal therapy of a mandibular first molar with five root canals: A case report. Iran Endod J. 2007;2:110-2.
- [Google Scholar]
- Incidence, and position of the canal isthmus. Part 1. Mesiobuccal root of the maxillary first Molar. J Endod. 1995;21:380-3.
- [CrossRef] [PubMed] [Google Scholar]
- To assess the occurrence of middle mesial canal using cone-beam computed tomography and dental operating microscope: An in vitro study. Journal of Conservative Dentistry: JCD. 2020;23(1):51.
- [CrossRef] [PubMed] [Google Scholar]
- Cone beam computed tomography (CBCT) in endodontics. Dent Update. 2010;37:373-9.
- [CrossRef] [PubMed] [Google Scholar]
- Accuracy of CBCT, digital radiography and cross-sectioning for the evaluation of mandibular incisor root canals. Iran Endod J. 2016;11:106-10.
- [Google Scholar]




