

Translate this page into:
TREATMENT OF CLASS I MALOCCLUSION WITH LOWER INCISOR EXTRACTION
Corresponding Author : Dr. Rashi Chauhan
This article was originally published by Indira Gandhi Institute of Medical Science and was migrated to Scientific Scholar after the change of Publisher.
Abstract
The extraction of the lower incisor constitutes a therapeutic alternative in treating certain anomalies. It is not a standard approach to symmetrically treating most malocclusions, but in certain clinical situations the therapeutic aims must be adjusted to individual patient needs - even when this means that achieved final occlusion is not ideal. A case report is presented with one mandibular incisor extraction treatment of a 17 year-old male with a Class I malocclusion that shows a significant mandibular arch length deficiency and mandibular tooth-size excess. In this case, the degree of mandibular anterior dental crowding, existing mandibular tooth-size excess indicated the extraction of one mandibular incisor.
Keywords
Mandibular incisor extraction
Bolton discrepancy.

INTRODUCTION:
Many approaches for crowded mandibular anterior teeth are currently employed: distal movement of posterior teeth, lateral movement of canines, labial movement of incisors, interproximal enamel reduction, removal of premolars, removal of one or two incisors, and various combinations of the above. Selecting the best treatment is often difficult, and all guidelines do not apply to every case1.
Treatment by extraction of one single mandibular incisor is not popular in the orthodontic profession despite the apparent advantages of the extraction in the region of crowding2,3. This treatment option may be indicated in malocclusions with anterior tooth size discrepancy due to narrow maxillary incisors and/or large mandibular incisors. It is contraindicated in malocclusions without anterior discrepancy or with discrepancies caused by large maxillary incisors and/or narrow mandibular incisors. The literature suggests this method affords improved post-treatment stability compared with premolar extraction.
Objections to this extraction option have been based on case reports or subjective clinical opinions after observing less desirable outcomes in treated Class I and Class II malocclusions1,4,5,6. Unwanted side-effects have been increase of overbite and overjet beyond acceptable limits, space reopening, partly unsatisfactory posterior occlusion, recurrence of crowding in the remaining three incisors, and unaesthetic loss of the interdental papillae in the mandibular anterior region1,4,5,6,7,8.
Prior to choosing the most favourable treatment option it is important to analyze treatment goals, stability, the final occlusion to be achieved and the esthetic conditions that constitute a case. In view of this fact, lower incisor extraction becomes an alternative treatment for malocclusions that do not fit the conventional forms of extraction since they are more stable in the long term9. A diagnostic setup is strongly recommended with this treatment approach. The main indication to extract a lower incisor is the presence of tooth size discrepancy equal to or greater than 3.5 mm due to lower anterior excess or upper anterior deficiency9-11. As pointed out by Kokich and Shapiro (1984), the deliberate extraction of a lower incisor in certain cases allows the orthodontist to improve occlusion and dental aesthetics with a minimum of orthodontic action.
Specific criteria for mandibular incisor extraction1,7,10 include:
Permanent dentition
Minimal or no growth potential
A Class I molar relationship
A harmonious soft-tissue profile
Minimal-to-moderate overbite
Little or no crowding in the maxillary arch
An existing Bolton discrepancy
A tooth-size-arch-length discrepancy of more than 3 mm in the anterior region.
Following the decision to extract one lower incisor, professionals must define which one to remove. Indication depends on a combination of the following factors: type of malocclusion, amount of anterior tooth size discrepancy, arch length deficiency in the anterior region, dental and health conditions of the supporting tissue and upper and lower dental midline relationship10. Extraction of a lateral incisor is generally preferred because it is less visible from the front10, but the incisor that is farthest outside the natural arch and closest to the crowding is usually the best candidate for extraction.
ADVANTAGES:
It diminishes the risk of anchorage loss since there is a solid anchorage unit in the posterior segments12. It reduces retention time as the likelihood of relapse is decreased12. It provides space in the area of greater crowding in the pre-treatment stage5,13,14.
Mandibular incisor extraction allows a reduction in tooth volume, minimizing changes in profile while reducing treatment time4,15. It allows orthodontists to improve dental occlusion and esthetics through minimum orthodontic action4.
Because little retraction is required compared with premolar extraction therapy, the anteroposterior position of the mandibular incisors is not changed, allowing maintenance of a harmonious profile10.
Levin16 argues that lower incisor extraction:
Improves facial profile by reducing the appearance of "mandibular protrusion."
Enables easy alignment of the lower anterior teeth.
Establishes an esthetically pleasing and functionally effective overbite.
Properly positions upper anterior teeth with acceptable axial inclinations instead of having to procline them to enable the positioning of all lower anterior teeth.
CASE REPORT:
HISTORY AND DIAGNOSIS
A 17-year-old male came to the Department of Orthodontics & Dentofacial Orthopedics, Kothiwal Dental College & Research Centre for orthodontic treatment with the chief complaint of irregularly placed lower front teeth. Patient was having permanent dentition and had a symmetric face with a convex profile and posterior divergence (Fig. 1). He had no important dental and medical history.

- Pre-treatment extra-oral photographs
Intraoral examination showed that there was mild crowding in the upper arch and severe crowding in anterior region of the lower arch. In occlusion, he had a 5 mm over-bite and a 2 mm over-jet. There was Class I molar relationship present on both left and right side and crossbite was present i.r.t 25. Mandibular midline was shifted 2 mm to the left. No mandibular shift was detected on closure. The arch length deficiencies were 3 mm in the maxillary arch and 7 mm in the mandibular arch. A Bolton analysis showed 5 mm mandibular excess in total and 3.1 mm mandibular anterior excess (Fig. 2).

- Pre-treatment intra-oral photographs
Radiographic examination revealed that all the permanent teeth were present. Cephalometric evaluation showed that he had a skeletal Class I relationship with average growth pattern. The maxilla and the mandible were both orthognathic relative to the cranium. Patient was in CVMI 6 stage (Fig. 3).
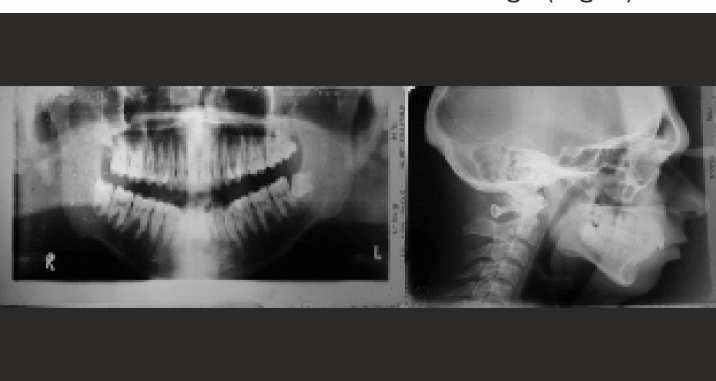
- Pre-treatment radiographs
TREATMENT OBJECTIVES
Relieving of upper and lower anterior crowding
Good and stable dentoalveolar changes
Maintenance of class I molar relation
To achieve ideal overjet/overbite
Maintenance of good profile
Crossbite i.r.t.25
TREATMENT PLAN:
Three approaches to the treatment of this malocclusion were considered - non extraction, four bicuspid extraction, and lower incisor extraction. Non-extraction was ruled out because of the severe lower arch length deficiency, the inadequate zone of attached gingivae labial to the lower right cuspid, and the risk of long-term instability.
It was believed that the extraction of four first bicuspids could result in excessive retraction of the uncrowded maxillary incisors, compromising the facial profile and incisor relationships.
Considering these criteria, lower incisor extraction was planned along with expansion of maxillary and mandibular arch because of good facial profile, minimal space requirement.
In order to evaluate the possible effects of extracting one lower incisor, a waxed diagnostic setup was constructed. This showed that satisfactory occlusal relationships could be achieved. This approach was finally selected because it could alleviate the lower arch length deficiency without affecting the facial profile.
In this case, blocked out lower right lateral incisor was selected for extraction. Upper space requirement was minimal and expansion was sufficient in achieving good result.
TREATMENT MECHANICS
A corrective standard Edgewise appliance (0.022 × 0.028-in slot) was set up and the patient underwent extraction of the lower right lateral incisor and expansion in the upper and lower arch with quad helix and bihelix respectively.
During correction mechanics the following was performed: alignment and leveling with 0.016-inch to 0.020-inch stainless steel wire, maintaining the posterior occlusion with passive bends, space closure through tie-back in the archwires, elastic chain and buccal (root) torque in the incisors. In the next step, 0.019 × 0.025-inch archwires were used in the upper and lower arches in a coordinated manner using forms and torques. Meanwhile, patient refused to go for further treatment as he has to go for training in front office in hotel management in other state. There was 2 mm of space present in between lower left lateral incisor and canine and some amount of intercuspation was also needed. The active treatment period was 12 months.
TREATMENT RESULTS:
Post-treatment facial photographs showed little change in facial profile (Fig. 4). The Class I molar relationship was maintained, and the mandibular crowding was corrected. The overjet was maintained, and the overbite was improved. Both arches showed good alignment, with the upper midline centered on the middle of the lower incisors. Incisor angulations were acceptable (Fig. 5).

- Post-treatment extra-oral photographs

- Post-treatment intra-oral photographs
The post-treatment cephalometric tracings showed minimal change in the soft tissue profile. The lower arch length deficiency was alleviated. Post-treatment radiographs showed that minimal root resorption had occurred during treatment and that root parallelism was satisfactory (Fig. 6) (Table 1).

- Post-treatment radiographs
| Pre-treatment | Post-treatment | |
|---|---|---|
| Skeletal analysis | ||
| S-N-A (°) | 84 | 83 |
| S-N-B (°) | 80 | 79 |
| A-N-B (°) | 4 | 4 |
| S-N/Go-Gn (°) | 30 | 30 |
| Posterior/Anterior ratio (%) | 66.6 | 66.6 |
| N-Me (mm) | 123 | 123 |
| S-Go (mm) | 83 | 83 |
| Wits appraisal | -2 | -1.5 |
| Dental analysis | ||
| Upper incisor to N-A (mm) | 5 | 4 |
| Upper incisor to N-A (°) | 27 | 25 |
| Upper incisor to A-Pg (mm) | 8 | 7 |
| Lower incisor to N-B (mm) | 5 | 4 |
| Lower incisor to N-B (°) | 26 | 26 |
| Lower incisor to A-Pg (mm) | 3 | 3.5 |
| IMPA (°) | 94 | 95 |
| Interincisal angle (°) | 128 | 128 |
| Overjet (mm) | 2 | 2 |
| Overbite (mm) | 5 | 4 |
| Upper intercanine width (mm) | 32.5 | 35.5 |
| Upper interpremolar width (mm) | 36 | 41.5 |
| Upper intermolar width (mm) | 48 | 52 |
| Lower intercanine width (mm) | 23 | 25 |
| Lower interpremolar width (mm | 29.5 | 33.5 |
| Lower intermolar width (mm) | 40 | 45.5 |
| Soft tissue analysis | ||
| Lower lip to E-line (mm) | 3 | 1 |
| Nasolabial angle (°) | 105 | 110 |
| Holdaway H angle (°) | 21 | 22 |
| Lower lip to E-line (mm) | 3 | 1 |
| Nasolabial angle (°) | 105 | 110 |
| Holdaway H angle (°) | 21 | 22 |
RETENTION:
Fixed bonded lingual retainer was given in relation to lower arch from canine to canine. In upper arch, Hawley's appliance was given.
DISCUSSION:
The rationale for extraction of a lower incisor in the case described was based on specific individual treatment objectives. In this case the results were enhanced or treatment was facilitated by protecting the supporting structures, decreasing the amount of tooth movement, minimizing facial change, and reducing treatment time.
Kokich and Shapiro consider a tooth-size analysis an important part of this evaluation. In some situations this may indicate little likelihood of a successful result with an incisor extraction, as in a case of significant maxillary anterior excess. On the other hand, if the analysis shows a lower anterior excess, the extraction of a lower incisor might have a positive effect4.
Reidel9 has suggested that in patients with severely crowded mandibular arches, the removal of one or more mandibular incisors is the only logical alternative which may allow for increased stability of the mandibular anterior region without continuous retention17.
Neff18 reported that he prefers to extract the lateral incisor in the belief that the distal face of a central incisor has better contact with the mesial surface of the canine. He further explains that when extracting a central incisor, contact occurs between the mesial surface of the remaining central incisor and the mesial surface of the lateral incisor, and even if the teeth are perfectly upright and parallel, sometimes an undesirable black triangle remains between the middle third of the tooth and the gingiva.
Valinoti1 suggested in 1994 that the extraction of a lower incisor is less likely to exhibit crowding relapse after retention because the incisor is located closest to the area where the problem is located, requiring less movement and effort to be exerted on the original conditions of the other teeth.
CONCLUSION:
Although the indications for this type of extraction decision are relatively rare, the possibility of incisor extraction should be a part of every clinician's portfolio of treatment techniques. One single mandibular incisor extraction can be an effective treatment choice for the appropriate malocclusion with a Bolton discrepancy. In patients with moderate crowding and without excessive mandibular tooth mass, interproximal reduction may be a better alternative. If it is carefully planned and executed in the proper situation, incisor extraction can be an effective way of satisfying a particular set of treatment objectives. Minimal alteration of mandibular arch form is the key for success and stable results.
REFERENCES:
- Mandibular incisor extraction therapy. Am J Orthod Dentofacial Orthop. 1994;105(2):107-16.
- [CrossRef] [PubMed] [Google Scholar]
- JCO study of orthodontic diagnosis and treatment procedures. Part I: Results and trends. J Clin Orthod. 1996;30:615-629.
- [Google Scholar]
- Orthodontics. Part 8: Extraction in orthodontics. Br Dent J. 2004;196:195-203.
- [CrossRef] [PubMed] [Google Scholar]
- Lower incisor extraction in orthodontic treatment. Four clinical reports. Angle Orthod. 1984;54(2):139-53.
- [Google Scholar]
- The mandibular central incisor, an extraction option. Am J Orthod Dentofacial Orthop. 1997;111(3):253-9.
- [CrossRef] [PubMed] [Google Scholar]
- Mandibular incisor extraction: indications and long-term evaluation. European Journal of Orthodontics. 1996;18:485-489.
- [CrossRef] [PubMed] [Google Scholar]
- The long term effects of one lower incisor extraction. Eur J Orthod. 1985;53:706-713.
- [Google Scholar]
- Mandibular incisor extraction: post-retention evaluation of stability and relapse. Angle Orthod. 1992;62(2):103-16.
- [Google Scholar]
- Lower incisor extraction in orthodontic treatment. Am J Orthod. 1977;72(5):560-7.
- [CrossRef] [PubMed] [Google Scholar]
- An evaluation of changes in mandibular anterior alignment from 10 to 20 years post-retention. Am J Orthod Dentofacial Orthop. 1988;93(5):423-8.
- [CrossRef] [PubMed] [Google Scholar]
- Different extractions for different malocclusions. Am J Orthod. 1975;68(1):15-41.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of mandibular incisor extraction on anterior occlusion in adults with Class III malocclusion and reduced overbite. Am J Orthod Dentofacial Orthop. 1999;115(2):113-24.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of a Class III malocclusion with a missing mandibular incisor and severe crowding. Am J Orthod Dentofacial Orthop. 1999;116(6):661-6.
- [CrossRef] [PubMed] [Google Scholar]
- Retention and stability: A review of the literature. Am J Orthod Dentofac Orthop. 1998;114:299-306.
- [CrossRef] [PubMed] [Google Scholar]
- The size relationship between the maxillary and mandibular anterior segments of the dental arch. Angle Orthod. 1957;27(3):138-47.
- [Google Scholar]




