

Translate this page into:
SURGICAL REMOVAL OF A RARE ODONTOGENIC TUMOR WITH AN IMPACTED CANINE FROM MAXILLA-A CASE REPORT AND REVIEW OF LITERATURE
Corresponding Author : Dr. Soubhik Pakhira
This article was originally published by Indira Gandhi Institute of Medical Science and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract: Odontogenic tumors exhibit different kind of histopathological features which are pertinent to the different stages of tooth development. The biologic behaviour of these lesions is varied from a hamartomatous lesion to a benign neoplasm or even to an aggressive malignant tumor. Ameloblastic fibro-odontomas (AFO) are benign mixed odontogenic tumor of the jaws. There are frequently considered together with ameloblastic fibroma because they appear to be slight variations of the same benign neoplastic process. A case of an ameloblastic fibro-odontoma of anterior maxilla is reported with relevant review of literature of clinicopathologic correlations.
Keywords
Ameloblastic fibro-odontoma (AFO)
Ameloblastic fibroma
Odontoma
Odontogenic tumor
Maxillary canine
Ectomesenchyme

INTRODUCTION:
Ameloblastic fibro-odontoma (AFO)is a rare odontogenic tumor composed of morphologic features characteristic of ameloblastic fibromas on the one hand and complex odontomas on the other.1 The biologic behavior of ameloblastic fibroma, ameloblastic fibroodontoma and odontoma is often similar. They are benign mixed odontogenic tumors composed of neoplastic epithelium and mesenchyme with microscopically identical soft tissue components. The pathological entity has been classified by WHO (World Health Organization) under the odontogenic epithelium with odontogenic ectomesenchyme with or without hard tissue formation.2 Ameloblastic fibroodontoma (AFO) has been defined by the WHO classification as “a lesion similar to ameloblastic fibroma, but showing inductive changes that lead to formation of dentin and enamel”.3,4 The AFO is a well-circumscribed, painless, slow-growing, and expanding tumor with no propensity for bony invasion. It tends to produce swelling and has a central location in the jaws. In the majority of cases the AFO is associated with an unerupted tooth.1 Here a case of AFO is reported with reviews of relevant clinicopathological features of the neoplasm.
CASE REPORT:
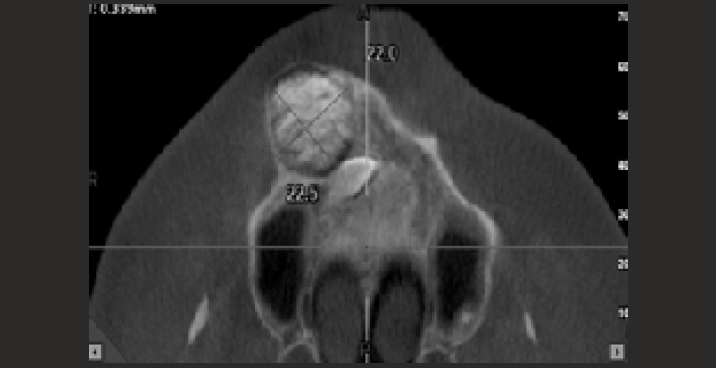
An 18-year-old male patient was referred to the Department of Oral and Maxillofacial surgery of Dr. R. Ahmed Dental College and Hospital with chief complaint of a swelling and occasional pain in his right upper jaw in front teeth region. The swelling had a bulged-out appearance causing obliteration of nasolabial furrow in extraoral appearance (Fig:1). A bony hard swelling found at the right canine fossa region with missing of maxillary right canine and retained right deciduous cuspid (Fig:2). The swelling was roughly ovoid in shape with approximate mean diameter of 2 cm. There was no history of discharge, local trauma or infection and there was no other clinical finding. The medical, social and family histories were unremarkable. CBCT (Cone-beam computed tomography) examination revealed a radiopaque mass of irregular outline with a well-defined radiolucent border causing divergence of roots of regional teeth (right lateral incisor, right first premolar) and resorption of outer cortex of buccal bone. The maxillary right canine was found impacted horizontally in posterosuperior positionof the lesion (Fig:3, Fig:4). The axial view of CBCT revealed that the lesion had diameter of 22.5mm × 22.0mm (Fig:3).


The differential diagnosis included immature complex odontoma, calcifying epithelial odontogenic tumour, adenomatoid odontogenic tumour, calcifying epithelial odontogenic cyst and ameloblastic fibro odontoma.
The lesion was planned for enucleation under local anaesthesia with simultaneous removal of impacted maxillary right canine. The routine investigations of the patient were within normal ranges.
The lesion was exposed after raising a trapezoidal flap after achieving local anaesthesia. The hard mass was found to be encapsulated by a well-defined cystic lining. The mass was enucleated in toto by means of a blunt instrument. After removal of the encapsulated mass the impacted right maxillary canine was removed by means of decapitation. It was done with utmost care as the canine was buried in close vicinity to nasal aperture. After achieving haemostasis, the site was closed primarily by interrupted sutures.
The enucleated hard mass was examined in vitro and it was found to be chalky in consistency (Fig:5, Fig:6). The specimen was sent for histopathological evaluation to the Department of Oral and Maxillofacial Pathology.


The patient was called for follow up on 7th day and it showed uneventful soft tissue healing.
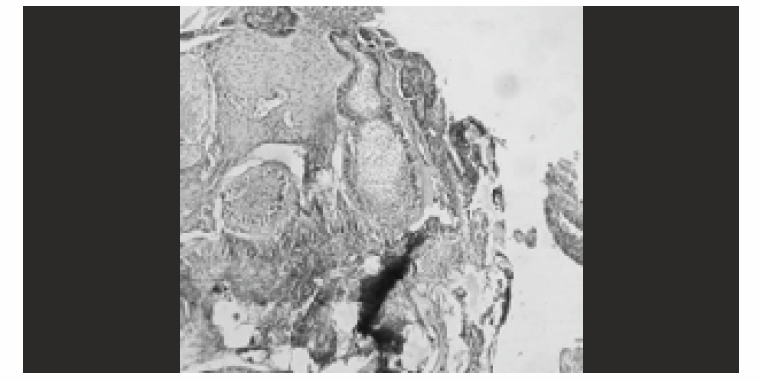
The histopathological report revealed presence of narrow cords and small islands of odontogenic epithelium in loose primitive appearing connective tissue. The calcifying element consisted of foci of enamel and dentin matrix formation in relation to epithelial structures (Fig:7). The overall histopathological features were suggestive of ameloblastic fibro-odontoma (AFO). No recurrence observed on follow up after one year.
DISCUSSION:
AFO first was delineated in 1972 by Hooker. 5A literature review of 50 cases of AFOs was published by Slootweg in 1981. These neoplasms occur predominantly in children and young adults. AFO usually is diagnosed in the first 2 decades of life, and about 98% of the tumors occur before the age of 20. Philipsen et al reported that the average age in 86 cases was 9 years. AFO is histologically composed of three predominant elements (1) immature fibroblastic connective tissue, (2) ectodermal component, and (3) mineralized component.6,7 The posterior mandible is affected 2.4 times more often than the entire maxilla. The AFO seems to occur exclusively as a central intraosseous tumor. Clinically, an AFO appears as a well-encapsulated, benign lesion, and it is frequently asymptomatic. Radiography shows a well-defined, radio lucentarea containing various amounts of radiopaque material of irregular size and form. The tissue masses of an AFO show the characteristic structure of an immature complex odontoma consisting of irregularly arranged enamel, dentinoid, cementum, and pulplike ectomesenchymal tissue. At the tumor periphery, next to the fibrous capsule, there is a zone of strands and islands of odontogenic epithelium embedded in typical cell rich ectomesenchyme. Dentin production takes place toward the centre of thelesion.1 With the obvious difficulty of distinguishing between a true tumour and a developing odontoma that may at one stage exhibit the histological appearance of an ameloblastic fibroma or AFO. Furthermore, there is no consensus as to whe ther these tumours are separate entities or are different stages in the maturation of the same entity. AFO usually does not show aggressive behaviour as suggested by many clinicians and it can be treated adequately by surgical curettage and removal of the tooth. Malignant transformation from AFO is usually infrequent. Herzog et al. (1991) reported the case of a 14-year-old girl with an AFO that evolved into an odontogenic sarcoma.8 A case of extensive pigmentation was reported by Kitano et al. Where the authors observed abundant deposition of melanin widely distributed in the nests of the odontogenic epithelium. Aggregations of large melanophages similar to nevus cells were noted.9 A case of multiple AFOs in a father, his two sons, and a daughter was reportedby Schmidtseder and Hausamen. In addition to multiple AFOs, oesopha-gealstenosis, hepatopathy, dyspepsia. and increased-susceptibility to infection were observed. The case was suspected as a dominant autosomal inherited disorder.10Recurrence of AFO is infrequent as reported by most of the authors, which justifies more conservative approach in treatment.
CONCLUSION:
The presented case in the report was clinically, radiographically and histopathologically proven as a typical AFO. With the help of CBCT the location and extent of the lesion was determined precisely prior to the planning of its surgical removal. Interestingly impacted maxillary canine was found with the lesion as reported in various literature. Probably the expansile nature of the lesion was responsible for divergence of roots of regional teeth and displacement of the impacted maxillary canine more towards nasal aperture in cephalad direction. Surgical removal of the impacted canine was done after enucleation of the lesion with an idea that the tumour may arise from the remnant of odontogenic ectomesechyme tissues of the impacted tooth. The case was followed up after one year showing good bony and soft tissue healing without any recurrence. Early diagnosis and proper surgical planning proved to be keystone for achieving minimum tissue damage during surgery and more or less uneventful healing in post-operative period.
REFERENCES:
- Odontogenic tumors and allied lesions. Quintessence publishing; 2004.
- World Health Organization Classification of Tumours. In: Pathology and Genetics of Head and Neck Tumours. Lyon, France: International Agency for Research on Cancer (IARC); 2005.
- [Google Scholar]
- The WHO histologicaltyping of odontogenic tumours. Cancer. 1992;70:2988-94.
- [CrossRef] [PubMed] [Google Scholar]
- Ameloblastic odontoma, an analysis oftwenty-six cases. Oral Surg Oral Med Oral Pathol. 1967;24:375-6.
- [CrossRef] [Google Scholar]
- An analysis of the interrelationshipof the mixed odontogenic tu mors-a meloblastic fibroma, and theodontomas. OralSurg Oral Mad Oral Pathol. 1981;51:266-276.
- [CrossRef] [PubMed] [Google Scholar]
- Mixed odontogenictumors and odontomas: considerations on interrelationship.Review of the literature and presentationof 134 new cases of odontomas. Oral Oncol. 1997;33:86-99.
- [CrossRef] [PubMed] [Google Scholar]
- The ameloblasticfibro-odontoma e an odontogenic mixed tumor progressing intoan odontogenic sarcoma. Dtsch Z Mund Kiefer Gesichtschir. 1991;15:90e93.
- [Google Scholar]
- Pigmentedameloblastic fibro-odontorna with melanophages. Oral Surg Oral Med Oral Patho. 1994;77:271-275.
- [CrossRef] [PubMed] [Google Scholar]
- Multiple odontogenictumors and otheranomalies. Oral Surg OralMed Oral Pathol. 1975;39:249-258.
- [CrossRef] [PubMed] [Google Scholar]




