

Translate this page into:
NEWER GINGIVAL RETRACTION MATERIALS: A REVIEW
Corresponding Author : Dr. Neha Vaidya
This article was originally published by Indira Gandhi Institute of Medical Science and was migrated to Scientific Scholar after the change of Publisher.
Abstract
The factors responsible for the longevity and aesthetics of a restoration are intimately linked to the gingival and periodontal tissues. The placement of any restoration placed in close proximity to the gingival tissues requires adequate access and isolation, for which various gingival retraction methods and materials are available. These are classified broadly as mechanical, chemo-mechanical, cordless and surgical techniques. This review focuses on the rationale behind gingival retraction and a discussion of the newer modalities developed in this regard.
INTRODUCTION:
During various procedures like impression or luting of the restorations, multiple challenges can surface. Moisture control plays a pivotal role for any dental procedure- direct or indirect. This is achievable only in case of effective isolation techniques. Numerous problems are faced in operative dentistry. These can range from the limiting influence of all the associated muscles to other hindrances manifested due to limited vision and isolation, which can be a result from of crevicular fluid, saliva and gingival bleeding during tooth preparation to receive a restoration. The retraction of the gingival tissue is a long-established technique. It can be defined as the process of deflection of the marginal gingiva away from a tooth. Gingival retraction is aimed at accessibility of the impression material beyond the abutment margins and also to provide enough space for the impression material to be thick enough. This is because thickness of material has been found to affect its tear resistance. The present clinical condition will dictate the gingival retraction technique being used. Hemorrhage and its magnitude may incline towards a specific retraction technique.
NEED FOR GINGIVAL RETRACTION
To widen the gingival sulcus in order to provide access for impression material to reach the subgingival margins and to record adequately the finish line.
Helps in obtaining the perfect die with accurate margins, which helps in margin placement and contouring of the restoration.
Helps in blending of the restoration with the unprepared tooth surface.
Helps in placement and finishing of the margins on the prepared tooth.
During cementation it helps in easy removal of cement without tissue damage.
It helps the dentist in visually assessing the marginal fit and any caries if present.
In situations when it is necessary to extend the restoration below the gingival margin to enhance retention.
To enhance access and to prevent damage to the soft tissue during cavity preparation procedure, it may be desirable to carry out some degree of gingival retraction prior to commencement of preparation
METHODS FOR GINGIVAL RETRACTION:
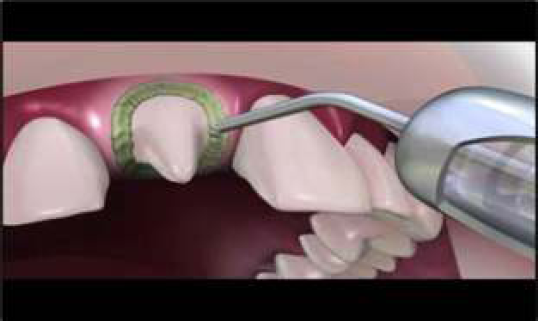
Method which is used most commonly for retraction of gingival is retraction cord (can be combined with different chemical solutions and gels with astringent or hemostatic action). Other commonly used methods include electrosurgical units, soft tissue diode lasers and retraction pastes. A combination of these techniques can also be used. Although gingival cord is more readily used, but it can damage the delicate epithelial lining of the sulcus and underlying connective tissues.9,10
Hence, focus is being shifted to newer methods for gingival retraction. Some of them include:
EXPASYL:
Expasyl (Kerr Corporation, Orange, CA) is a clay- like material that is dispensed from a syringe apparatus through a narrow needle-like tip.
It is available in vials and dispensed directly into the sulcus with a heavy-duty delivery gun loaded with a syringe. Expasyl has no chemical or setting reaction. It does not go through an expansion phase.
The material is left in place for up to 2 min and is then rinsed off with an air/water syringe. The sulcus is then ready for the impression. The material contains aluminum chloride, a potent hemostatic agent. Hence, no violation occurs to the gingival complex.
Gingival recession is also not encountered. After removal of Expasyl, sulcus is clean which reduces artifacts during making of digital CAD/CAM impressions. It provides the best outcome of chemical choices available.
Compositions:
Kaolin 66.75%
Aluminum chloride 6.54%
Oil of lemon 0.33%
Water 25.36%
Colorant 1.02%
pH = -3.
Advantages:
Minimal or no physical damage to the gingival tissues.
Time saving in situ actions where multiple teeth are being impressed
Minimal cost
Predictable hemostasis is achieved.
DISADVANTAGES:
More expensive
Inhibits set of polyvinyl siloxane and polyether impressions
Less effective with very subgingival margins.
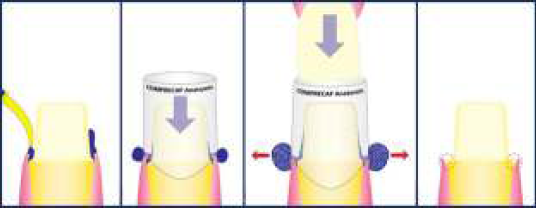
MAGIC FOAM CORD:
Magic foam cord is a new non-hemostatic method.
It is a vinyl polysiloxane material designed for retraction of the gingiva.
The material is syringed around the margins of tooth preparation and pressure is maintained using a cap.
The material expands, and after 5 min, impression can be made. The material expands (160%) after 5 min
Advantages:
Less traumatic to tissues than retraction cord
Color of foam makes it easy to see during use
Easy to remove material from preparation and sulcus
Adequate working time.
Perfect retraction of the Sulcus, stops bleeding without invasive materials or techniques
Easier to use (same as impression making). Flows directly into the Sulcus. No need for technique sensitive application technique.
Astringent is not required - no need to rinse
More efficient - when doing multiple preparations
Disadvantages:
No hemostasis provided
Expensive when compared to cord
No improvement in speed or quality of retraction compared to cord
Less effective on subgingival margins
Intraoral tips too large to inject material adequately into the sulcus.
MATRIX IMPRESSION SYSTEM:
Matrix impression system is a new system in which impression procedure includes three steps:
First, a matrix of polyether occlusal registration elastomeric material is done over the prepared tooth.
The retraction cord is removed and a definitive impression is recorded in the matrix using a high viscosity elastomeric impression material.
After the matrix impression is positioned, medium viscosity elastomeric material is loaded in an impression tray and is seated over the matrix and remaining teeth to create impression of the entire arch.
The design of the matrix also forces the high viscosity impression material along the preparations and into the sulcus. The matrix impression system uses three impression materials of different viscosities.
Advantages:
Eliminates chances of tearing of the sulcus
Cleans blood and debris from the sulcus area
Delivers impression material in the gingival sulcus slowly and with more accuracy and speed
Holds the sulcus open for an increased time.
Disadvantages:
Increased chairside time.

(a) Tooth surface after final preparation. Clean the tooth surface and ready for impression.
(b) (c) Cut off 1 to 2mm of the impression tip to apply bite registration material to fill the margin area and cover the teeth.
(d) Wait until the bite registration material setting, remove it carefully.
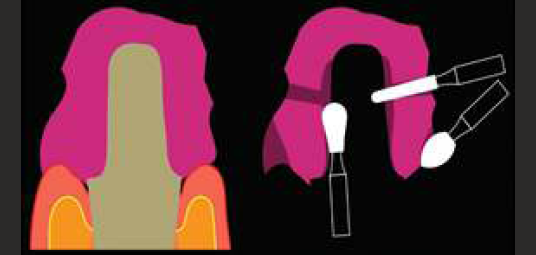
a) The figure shows how does the bite registration material adapts on the tooth and fills the gingival margin. b) There are three critical features while trimming the matrix.

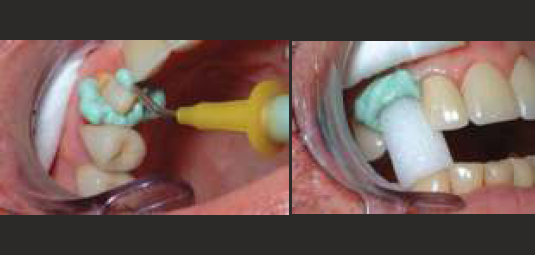
a) After trimming the matrix, use the air-water spray to clean the dust off. b) This figure shows the appearance of the finished matrix.

a) b) Apply light body or medium body impression material onto teeth and inside the matrix. c) Place the matrix onto the abutment teeth. d) Pick-up impression with stock tray and medium body PVS.

a) b) The final impression result and close-up view. c) The working cast and die. d) The final result of the anterior six crowns.
ADVANTAGES:
Eliminates chances of tearing of the sulcus
Cleans blood and debris from the sulcus area
Delivers impression material in the gingival sulcus slowly and with more accuracy and speed
Holds the sulcus open for an increased time.
DISADVANTAGES:
Increased chairside time.
MEROCEL STRIPS:
Merocel is a new retraction material to displace gingiva with no tissue injury before making impression.
Merocel retractions strips are synthetic material, which are specifically chemically extracted from a polymer hydroxylate polyvinyl acetate that creates a net-like strip without debris or free fragments.
Placement of Merocel retraction technique does not require use of local anesthesia.
Merocel retraction strip provides very excellent gingival retraction when compared to conventional retraction cord.
The porous and sponge-like microstructure of Merocel produces a dry field for the impression to accurately capture the details. The absence of fibers decreases the risk of postoperative problems.
Advantages:
It is shaped easily
It effectively absorbs oral fluids
The sulcus is clean without the presence of any debris.

A gingival finish line is prepared within the intracrevicular space. A 2 mm thick Merocel retraction strip is inserted
The patient is asked to maintain pressure on the artificial crown for 10 to 15 minutes. The Merocel retraction strips tend to expand with absorption of selected oral fluids, exerting pressure on surrounding tissues to provide gingival retraction.
The material in the intracrevicular space is removed and an impression is made.
GINGITRAC:
Gingitrac is a paste system that uses a syringe to apply the paste around the margins.
The syringe is preloaded with the paste.
The paste contains aluminum sulfate as an astringent. If necessary, a hemostatic agent can be applied before its use.
The cap is first filled with the paste and then placed over the tooth for 5 min. The paste is applied with a syringe in the sulcus.
For impressions of more than one tooth, a plastic tray is used to carry a firm paste matrix over which the Gingitrac paste is syringed.
The tray is then positioned and removed after 3-5 min. For both single and multiple tooth preparations, retraction of gingiva is by pressure application. The paste is removed prior to impression making.
Advantages:
Easier to express from automix gun
Longer shelf life
Faster setting time
Controls oozing of blood
Removal is fast and easy
Materials slip cleanly out of sulcus without trauma.
STAY PUT:
Stay put combines the advantages of both an impregnated and braided cord with the adaptability of an ultrafine copper filament. Aluminum chloride hexahydrate is used for impregnation. Nonimpregnated stay put cord is also available which can be impregnated with hemostatic agent as needed.
The pliable core is so effective that the cord is not only easy to place in the sulcus but it stays there.
Features & Benefits:
Can be preformed
Does not unravel
Easily adapted
Stays in sulcus
No overlapping required
Advantages:
Hemostasis is fast
Possible to be preshaped
Pliable and can be adapted
Relatively safe for cardiac patients.
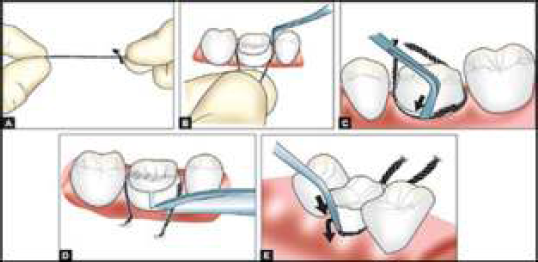
Direction to use stay put:
Cut Stay-put to the required length.
Stay-put can be soaked in any gingival retraction solution of your choice.
Place the center of the cord into the sulcus.
Leave the non-impregnated cord for at least 5 minutes in the sulcus.
When using GINGIVA LIQUID allow 1-3 minutes for the liquid to take effect.
Remove the cord directly before taking the impression
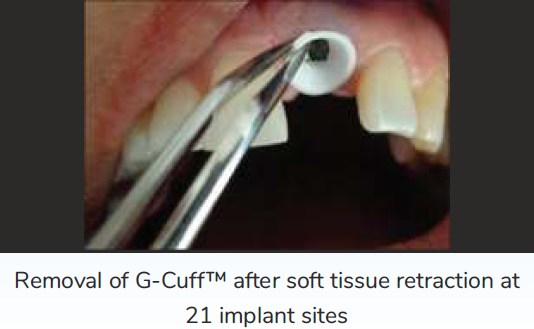
G-CUFF:
It is a disposable plastic collar launched by Canadian company, named Stomatotech, for the purpose of retraction of gingiva.
It is first inserted on the apical end of the abutment after which the abutment should be engaged to the implant.
The plastic collar is found between the apical part of the abutment and the gingival soft tissue.
The plastic collar should be drawn out and then removed permanently after retrieving the impression from the mouth.



LASER:

Use of lasers is adjunctive in fixed prosthodontics. The laser produces minimal damage of collateral tissue when laser energy of the correct wavelength is used.
Neodymium: yttrium-aluminum-garnet lasers are not used as their use can result in loss of bone.
Erbium: yttrium-aluminum-garnet (Er: YAG) lasers are fairly safe to use as they penetrate soft tissues minimally. CO2 lasers are used around implants. The primary chromophore for CO2 lasers is H2O. These lasers take in less energy close to metal implant surfaces, producing less temperature increases (<3°C) and less collateral damages. The soft-tissue structure is not altered by these lasers.
Advantages:
Excellent hemostasis is provided by CO2 laser
There is reduced shrinkage of tissue
There is comparatively less pain and the sulcus is also sterilized.
Disadvantages:
Er: YAG lasers are not good for producing hemostasis
CO2 laser provides no tactile feedback, leading to risk of damage to junctional epithelium.
CONCLUSION:
Finish line exposure in fixed prosthodontics is no longer difficult. Various advanced materials are available for gingival retraction. Using these materials, we can definitely improve the quality of impressions in fixed prosthodontics. Furthermore, the procedure can be relatively painless, quick, and atraumatic. The selection of material has to be carefully done by the operator. Since gingival retraction is an integral part of clinical practice, the clinician should make an effort to utilize different methods and products available for retraction of gingival tissues in various clinical scenarios. Sometimes a combination of methods may be needed, and some things may work for one clinician and not for another. The effort put into the appropriate retraction of gingival tissues pays off in terms of longevity of restorations, better margins and aesthetics.
REFERENCES:
- Gingival displacement for impression making in fixed prosthodontics: Contemporary principles, materials, and techniques. Dent Clin North Am. 2014;58:45-68.
- [CrossRef] [PubMed] [Google Scholar]
- Quick, painless, and atraumatic gingival retraction: An overview of advanced materials. J Pharm Bioallied Sci. 2016;8(Suppl 1):S5-S7.
- [CrossRef] [PubMed] [Google Scholar]
- The segmental impression technique: Astraight solution to a difficult problem. In: J Prosthet Dent. Epub ahead of print; 2019.
- [Google Scholar]
- The use of lasers in fixed prosthodontics. BDS, LDS RCS, MFGDP Private Practice, 30, East Parade, North Yorkshire, Harrogate, HG1 5LT, UK. Dental Clinics of North America. 2004;48:971-998.
- [CrossRef] [PubMed] [Google Scholar]
- GingiTrac™ [Internet] Centrix Dental. Available from: https://www.centrixdental.com/gingitrac-retraction-system.html. [cited 2018 Dec 06]
- [Google Scholar]
- The matrix impression system for fixed prosthodontics. Journal of Prosthetic Dentistry. 1998;79:208-16.
- [CrossRef] [PubMed] [Google Scholar]
- The intracrevicular restorative margin, the biologic width and the maintenance of the gingival margin. International Journal of Periodontics & Restorative Dentistry 1984:431-49.
- [Google Scholar]




