

Translate this page into:
A NEW APPROACH FOR PLANNED UPPER INCISOR POSITION - AN OBSERVATIONAL PROSPECTIVE STUDY"
Corresponding Author : Dr. Prema Anbarasu
This article was originally published by Indira Gandhi Institute of Medical Science and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
The profile of the patient is judged many a times by the position of the anterior teeth. Maxillary incisor labiolingual inclination and anteroposterior position play an essential role in the esthetics of the smiling profile. Hence the aim of the present study is to determine the planned incisor position in relation to the third palatal rugae an immutable landmark in the oral cavity
Materials and methods:
The study group consists of 80 participants consisting of 40 males and 40 females who satisfied the Andrew's six keys of occlusion. The impression of the upper dental arch was made using alginate impression material and the study casts were prepared with dental stone. The rugae pattern was marked on the study cast and the horizontal distance between the third palatal rugae to the incisal edge of upper incisor was measured using digital offset centerline Vernier caliper. The profile photograph of the participants was taken to verify skeletal class I relationship. The data collected were statistically analyzed using SPSS program.
Results:
The measured value between third rugae and incisal edge was 16-20 mm for females and 19-21mm for males. Therefore the planned incisor position for females is between 16-20 mm and 19-21mm for males.
Conclusion:
Knowing the ideal distance between the maxillary incisors and the third palatal rugae will help the orthodontist to plan the final anteroposterior position of the maxillary incisors during treatment.
Keywords
Incisor Position
Palatine Rugae
Ideal Profile.

INTRODUCTION:
Although orthodontic treatment is based mainly on occlusal relationships, great attention has been paid in achieving optimal facial profile esthetics. In recent times, orthodontic treatment mechanics give importance to the upper incisor position and rest of the teeth are aligned in accordance with the position of the central incisors1. The profile of the patient is judged many a times by the position of the anterior teeth. Maxillary incisor labiolingual inclination and anteroposterior position play an essential role in the esthetics of the smiling profile2.
Malocclusion due to proclined incisors is the most common complaint among patients seeking orthodontic treatment. The treatment of severely proclined anterior teeth usually, requires a reduction in tooth material in the form of extraction of first premolars and with controlled movement of teeth leads to a normal facial profile esthetics3. With the advent of improved orthodontic and surgical techniques, emphasis has shifted more towards envisioning an ideal position of upper incisors as the starting point in the planning of the treatment. In modern orthodontics, there has been changes in the goals of orthodontics to focus more on facial proportions and the effects of the teeth position and occlusion on facial harmony and appearance.
Determination of ideal incisor position is a challenge to the orthodontist, since over retraction of incisors results in dished in faces and under retraction will also not provide appreciable improvement in facial esthetics. Hence, evaluation of Ideal Position of Maxillary central Incisors in relation to stable anatomic reference point in patients is of utmost importance.
Palatal rugae appear during the third month of intrauterine life and occupy most of the length of palatal shelves. These structures form a series of anatomical folds on the anterior part of the palatal mucosa, behind the incisive papilla on each side of the median palatal raphe4. The number varies from 4 to 6 on each side, and they appear before the fusion of the palatine shelves5. It is used in various fields such as sex determination, orthodontics and forensic odontology6. Palatal rugae also refer to a series of transverse ridges on the anterior part of the palate and these are present on both the sides of the mid-palatal raphe and behind the incisive papilla. Palatal rugae can be used to evaluate the dental movements in orthodontics.
Palatal rugae imparts a special role in the Orthodontics, they are used as stable reference landmarks for the superimposition of pre- and posttreatment cephalometric tracings7. They can be used in the identification of submucosal clefts and also to assess the amount of anteroposterior tooth movement post treatment.
Shukla et al, compare the stability of palatal rugae before and after orthodontic treatment and concluded that the lateral part of third palatal rugae were the most immutable and that it could be used as a reference to evaluate the change in teeth position during orthodontic treatment8. Hence the aim of this study is to determine the ideal upper incisors position in relation to third palatal rugae in patients with normal occlusion and normal facial profile.
MATERIALS AND METHODS:
This cross sectional study protocol was reviewed and approved by Institutional Human Ethics Committee(450/IHEC/3-19) dated 19-04-2019. The duration of the study was about 2 yrs from June 2019 to June 2021. The study participants include Undergraduate and postgraduate dental students, medical students, nursing staff, patient attendants etc. All the participants were explained about the study and that were screened to meet the inclusion criteria.
The inclusion criteria are the following:
Age ranging from 18-30 years.
Participants possessing all the (Andrews) six keys of occlusion.
Had harmonious and well balanced facial profile.
No H/o orthodontic treatment.
Those willing to participate in the study.
The exclusion criteria are the following:
Participants with any dentofacial syndromes.
Participants with facial asymmetry.
Participants with TMJ problem or ankylosis.
The sample size was determined by a previous study by Andrews LF in 2001 14 was calculated to be N = 80, with 95% power at 5% β- error. Eighty participants consisting of 40 males and 40 females satisfying both the inclusion and the exclusion criteria were selected for the study. The study was explained and a written consent was obtained from each of the participants. The impression of the upper dental arch of the selected participants was taken with high quality alginate impression material and the study casts were prepared in high quality dental stone. The rugae patterns was marked on the study cast using a pencil (Fig 1).

- Study cast to measure the palatal rugae - epper incisal horizontal distance
Digital offset centerline Vernier caliper is used for measuring the distance between the third palatal rugae and the incisal edge of upper incisor. A horizontal line is drawn from end of the lateral part of the third Palatine rugae to the mid palatal raphe. Then the distance between the point marked on the midpalatal raphe and the upper incisal edge is measured using digital offset centerline vernier caliper. In addition the profile photograph of the participants was taken to confirm class I skeletal relationship. The distance from the end of the lateral part of the Palatine rugae and the incisal edges are measured for all the participants and is included in the statistical analysis.
STATISTICAL ANALYSIS AND RESULT:
Data was analyzed using SPSS (version 22.0; SPSS, Inc., Chicago, IL, USA). Descriptive statistics, including means, medians, standard deviations, range and 95% CI for mean, were calculated. Student t test is used to find out the statistical significant. Frequency distribution analysis was done for each group (both males and females).
The measurement of the distance between the lateral part of the Palatine rugue and incisal edge of all the participants was recorded. The measured value between third rugae and incisal edge for female was 16 mm for 10 participants, 18 mm for 21 participants, 20 mm for 9 participants(fig. 2) and the measured value between third rugue and incisal edge for Male was 19 mm for 7 participants, 20 mm for 22 participants, 21 mm for 11 participants (fig. 3).
The statistical analysis shows 18 mm for females and 20 mm for males to be a significant value and can be considered as a standardized value for determining the planned upper incisor position (fig. 4, 5).
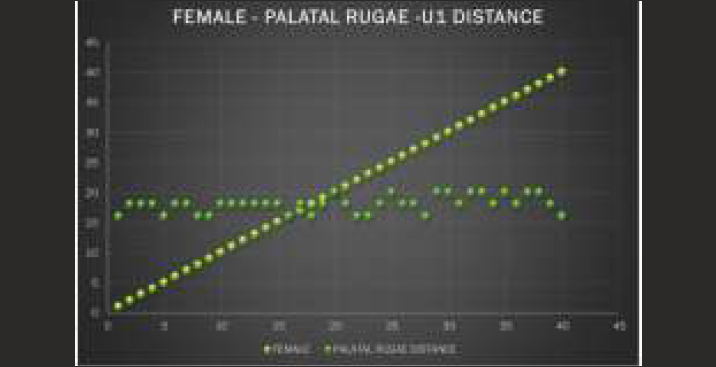
- Measured value palatal rugae -U1- female
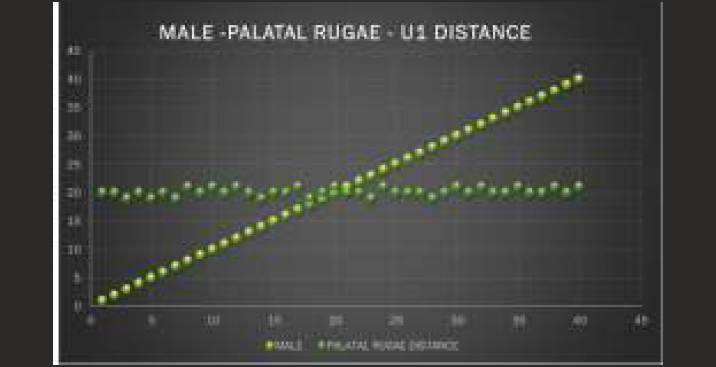
- Measured value palatal rugae -U1- male
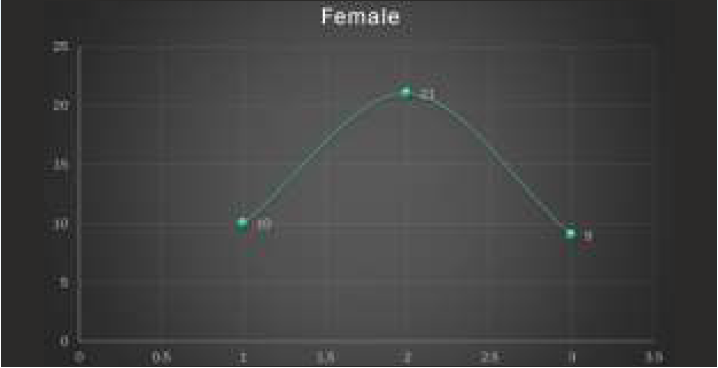
- Frequency distribution value - female
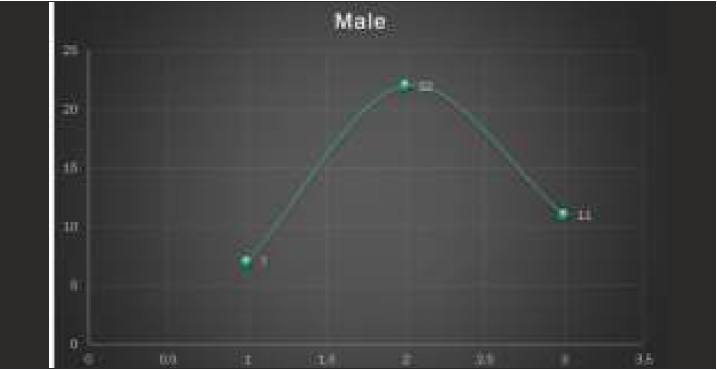
- Frequency distribution value - male
DISCUSSION:
This is a prospective observational study to determine the ideal incisor position in relation to Lateral part of third palatal rugae. Determination of the correct maxillary incisor position is very important in developing treatment plans for orthodontic patients. The AP position of the maxillary central incisors can be evaluated clinically using the palatal rugae as reference. The AP position of the maxillary central incisors between the male and female in the participants was found to be statistically significant. On average the palatal rugae distance to the maxillary central incisors in the male and female group were identified as 20 mm and 18 mm respectively. This study showed how the stable third palatal rugae can be used to evaluate the AP position of the maxillary central incisors.
Different approaches have been suggested to evaluate the maxillary incisor position, including traditional lateral cephalometric radiograph analysis and soft-tissue analysis.
Edward Ellis and Mcnamara et al9, evaluated upper incisor position using N-pog and they found a significant correlation. Arnett et al10 developed a soft tissue cephalometric analysis tool where they evaluated the planned incisor position for different soft tissue conditions which included lip thickness and lip support. Holdaway et al11 first suggested maxillary incisors as best teeth for esthetic prognosis as they determine upper and lower lip postures. Riedel et al12 first used N-pog as a reference line to evaluate the incisor position in place of A-pog as point A is a highly variable point. Nasion is also a variable point but it is more reliable than point a as maxilla is most affected by malocclusion. Alvarez A et al13 was not convinced regarding the stability of conventionally used landmarks to determine incisor position. He introduced A-line to assess the incisor position in untreated class I subjects and concluded that ideal tooth position is seen when the A-line touches or passes within 1mm of facial surface of maxillary central incisor. Andrews et al14, popularized the use of forehead landmark to assess the antero-posterior position of the upper incisors and found marked correlation between the forehead inclination and the prominence and position of upper central incisor position.
Adams M. et al15 evaluated photographs to compare the antero-posterior relationship of the maxillary central incisors to forehead in adult white males and found that the incisor was positioned between forehead facial axis and glabella. Similar study was done by will Alan Andrews et al16 in adult white females and concluded with similar results. Michael A. Webb and colleagues17 have evaluated upper incisor position as a determinant of ideal soft tissue profile and concluded that the incisors were positioned between forehead facial plane and forehead midpoint plane. More recently El Asmar R et al.18 evaluated the ideal position of the maxillary incisor relative to upper lip thickness.
Thus increased importance was given to anterior teeth position especially the incisor position to plan or to assess the Esthetic profile of the patient. The use of skeletal landmarks and intracranial reference lines to determine the ideal anteroposterior position of the maxillary incisors can be unreliable because of errors in identification of these landmarks and the variability in the position of intracranial reference lines between individuals. In addition, good facial harmony can exist within a wide range of cephalometric values and positioning the upper incisors according to skeletal guidelines may not necessarily result in a pleasing soft tissue profile Soft tissue landmarks such as the nose, lips and chin may not accurately reflect the position of the maxillary incisors because of the variability in their thickness and length.
In the present study we have evaluated that the incisor position using a stable landmark in the oral cavity, which is lateral part of third palatal rugae. Palatal rugae also refer to a series of transverse ridges on the anterior part of the palate that are present on both the sides of the mid-palatal raphe and behind the incisive papilla. Palatal rugae can be used to evaluate the dental movements in orthodontics. This imparts them a special role in the orthodontics, they are used as stable reference landmarks for the superimposition of pre- and post-treatment cephalometric tracings8. They can be used in the identification of submucosal clefts and also to assess the amount of anteroposterior tooth movement posttreatment.
Shukla et al8, compare the stability of palatal rugae before and after orthodontic treatment and conclude the lateral part of third palatal rugae were the most immutable and that it could be used as a reference to evaluate the change in teeth position during orthodontic treatment.
Different methods for the evaluation of palatal rugae on dental cast using Optocom software, Reflex metrograph, photographs and photocopies of dental cast have been used in the past for the evaluation of palatal rugae. Each of these methods requires a sophisticated instrument, device or software that is not acquired by many investigators and clinicians.
Kapali et al and Moran et. al19 used slide Vernier caliper to measure palatal landmarks. Digital Vernier caliper was used in the current investigation as it is user- friendly and can be used directly on dental cast; therefore, does not require cast digitization and particular expertise.
The AP positions of the maxillary central incisors were strongly associated with the stable landmarks used in this study and strongly correlated with palatal rugae distance in adult with good facial harmony.
The results of this study indicate that the palatal rugae distance can be used as a landmark to estimate the ideal position of maxillary central incisor in study cast. Using the palatal rugae distance as a primary landmark for AP incisor positioning avoids the potential pitfalls of relying on cephalometric analysis or repose soft tissue analysis.
Borderline cases have mild to moderate tooth size arch length discrepancy. The discrepancy is not much so that one can easily opt for extraction, and it is also not very less so that one can start the case without extraction. Because non extraction treatment can protrude the incisors and extraction can land up in dished in face. Therefore there is great divergence of opinion in the treatment of such patient. This dilemma of extraction or non extraction always troubles the orthodontist and requires a careful diagnosis. Palatal rugae can be considered reliable landmark to determine the ideal incisor position clinically and help us to determine how much retraction of incisors are required especially in borderline cases. Many studies have been done to identify the ideal incisor position with various hard and soft tissue cephalometric analysis. But Palatal rugae is one of the stable landmark in determining the upper incisor position both clinically in patient's and laboratory using models in orthodontics. This study will help us to determine the planned incisor position in extraction case. This analysis we developed can be an adjunct tool along with the other analysis to determine the planned upper incisor position.
CLINICAL SIGNIFICANCE OF THE STUDY
The findings from this study can be incorporated into routine orthodontic record taking, diagnosis and treatment planning. The inclusion of a study casts with the Palatal rugae and maxillary incisors distance to the set of diagnostic records as well as clinical evaluation of the smiling facial profile will allow achieving ideal position of maxillary central incisors in the face.
It is a quick and simple way to analyze a critical soft tissue landmark (palatal rugae) and hard tissue landmark (maxillary central incisor). Generic norms are created and specified to a patient.
The future study is to Compare and correlate the various factors those determining the upper incisor position by cephalometric analysis (U1 - NA= 4mm) and our palatal rugae- upper incisal distance analysis as well as to analyze and compare the results in post orthodontic treatment model with greater sample size.
CONCLUSION:
The results of the study led to the following conclusions:
Knowing the ideal distance between the maxillary incisors and the third palatal rugae (considered to be the stable anatomic landmark) will help the orthodontist to plan the final anteroposterior position of the maxillary incisors during treatment planning.
It will also be helpful to avoid over retraction of incisors during extraction orthodontic treatment which adversely affect the facial esthetics.
This study will help to clinically evaluate the incisor position during treatment progression. The present study gave clinical applicability of palatal rugae distance to determine ideal incisor position. Also the mean linear value to determine position of upper incisor in the inclusion population of male & female was 20mm and 18 mm respectively.
REFERENCES:
- Effect of maxillary incisor labiolingual inclination and anteroposterior position on smiling profile esthetics. The Angle Orthodontist. 2011;81(1):121-9.
- [CrossRef] [PubMed] [Google Scholar]
- The use of palatal rugae for the assessment of anteroposterior tooth movements. American Journal of Orthodontics and Dentofacial Orthopedics. 2001;119(5):482-8.
- [CrossRef] [PubMed] [Google Scholar]
- Shh signaling is essential for rugae morphogenesis in mice. Histochemistry and cell biology. 2011;136(6):663-75.
- [CrossRef] [PubMed] [Google Scholar]
- Individuality of human palatal rugae. Journal of forensic science. 1988;33(3):718-26.
- [CrossRef] [Google Scholar]
- Significance of palatal rugae in orthodontics. Journal of Orofacial Research 2013:202-9.
- [Google Scholar]
- Establishing the reliability of palatal rugae pattern in individual identification (following orthodontic treatment) The Journal of forensic odonto-stomatology. 2011;29(1):20.
- [Google Scholar]
- Cephalometric evaluation of incisor position. The Angle Orthodontist. 1986;56(4):324-44.
- [Google Scholar]
- Soft tissue cephalometric analysis: diagnosis and treatment planning of dentofacial deformity. American Journal of Orthodontics and Dentofacial Orthopedics. 1999;116(3):239-53.
- [CrossRef] [PubMed] [Google Scholar]
- A soft-tissue cephalometric analysis and its use in orthodontic treatment planning. Part II. American journal of orthodontics. 1984;85(4):279-93.
- [CrossRef] [PubMed] [Google Scholar]
- An analysis of dentofacial relationships. American Journal of Orthodontics. 1957;43(2):103-19.
- [CrossRef] [Google Scholar]
- The A line: a new guide for diagnosis and treatment planning. Journal of Clinical Orthodontics: JCO. 2001;35(9):556-69.
- [Google Scholar]
- Syllabus of the Andrews orthodontic philosophy. Syllabus of the Andrews orthodontic philosophy 2001:124-159.
- [Google Scholar]
- Anteroposterior relationship of the maxillary central incisors to the forehead in adult white males. ORTHODONTICS: The Art & Practice of Dentofacial Enhancement. 2013;14(1)
- [CrossRef] [PubMed] [Google Scholar]
- AP relationship of the maxillary central incisors to the forehead in adult white females. The Angle Orthodontist. 2008;78(4):662-9.
- [CrossRef] [PubMed] [Google Scholar]
- Upper-incisor position as a determinant of the ideal soft-tissue profile. Journal of clinical orthodontics: JCO. 2016;50(11):651-62.
- [Google Scholar]
- Evaluation of the ideal position of the maxillary incisor relative to upper lip thickness. American Journal of Orthodontics and Dentofacial Orthopedics. 2020;158(2):264-72.
- [CrossRef] [PubMed] [Google Scholar]
- Vertical growth-related changes in the positions of palatal rugae and maxillary incisors. American Journal of Orthodontics and Dentofacial Orthopedics. 2008;133(1):81-6.
- [CrossRef] [PubMed] [Google Scholar]




