

Translate this page into:
A COMAPARATIVE STUDY OF THE CLINICAL EFFICIENCY OF A CHEMO MECHANICAL AGENT, BRIX- 3000, ROUND BUR FOR CARIES REMOVAL. AN IN VIVO STUDY.
Corresponding Author : Dr. Akanksha Sood
This article was originally published by Indira Gandhi Institute of Medical Science and was migrated to Scientific Scholar after the change of Publisher.
Abstract
AIM:
To compare and evaluate the effectiveness of caries removal using two methods: a chemo mechanical agent, Brix3000 and conventional rotary instruments. This study also compared the difference in pain and discomfort caused by both the methods.
METHODOLOGY:
Owing o the power of the study, forty young participants aged between 20-30yrs, were enrolled in this study. The patient with a deep Class I carious lesion extending upto middle third of dentin and no symptoms were selected. The patients were randomly divided into 2 groups: Group I Brix3000 (n=20), Group II conventional method (n=20). Complete caries was excavated in both groups and then analyzed with tactile assessment. The parameters assessed were: pain, discomfort level throughout the procedure and mean time required for the treatment.
RESULTS:
The study showed that conventional rotary instrumentation method required significantly less time for caries removal (p = .001). but resulted in statistically higher pain score (p = .002) and discomfort to the patient as compared to the BRIX3000.
CONCLUSION:
These findings suggest that BRIX3000 is an excellent treatment option for caries removal with the same effectiveness and less trauma than the conventional method, inspite of it taking a longer time to remove the caries.
Keywords
Caries removal
minimally invasive dentistry
BRIX3000
chemo mechanical agents.

INTRODUCTION:
Dental caries is a very common global health problem.1 Dental caries may be defined as a bacterial disease of calcified tissues of teeth and is characterized by demineralization of the inorganic and destruction of the organic substance of the tooth. Histologically, carious tissue is divided into four distinct zones, three of which are clinically visible. The necrotic zone and contaminated zone containing microbial biofilm comprise the outer layer, which can be recognised clinically as soft mineralized tissue of the tooth. The microbial load in this necrotic zone is extremely high. The next zone is the demineralization zone, which has very few microorganisms, few nutrients, and an anaerobic atmosphere. Clinically, this zone is associated with leathery dentine. Finally, the translucent zone of a firm, softer dentine is found near the pulp. This zone is characterised by demineralization and the absence of microorganisms because microbial flora cannot penetrate this depth. As the caries process progresses, the dentin also experiences mineral loss and bacterial invasion, which in return produces secondary dentin to protect the pulp.2
Dental caries can be superficial or deep.3 Deep caries is defined as radiographic evidence of caries reaching the inner third or inner quarter of dentine with a risk of pulp exposure. Recent research on carious tissue management supports less invasive strategies.
Living pulp is vital for the maintenance of tooth homeostasis. A conservative approach can lead to a favorable diagnosis and help avoid injury due to iatrogenic causes.4 The conventional method for caries removal involves use of high-speed rotary instruments, which have proven to be effictive since ages. However, it is an invasive technique and it comes along with several drawbacks: over preparation of cavities, sensitivity, pain and possible damage to pulp tissue due to elevated temperature and pressure on the pulp. Fear and anxiety due to the noise created by rotary instruments and the need for anesthesia significantly affect the cooperation of the patient in the dental clinic. These factors are driving forces in the development of alternative techniques that can overcome the shortcomings of the traditional method.5 Most often, such situations not only make the patient delay the dental treatment but also sometimes avoid it altogether, which can result in caries progression.
Minimally invasive dentistry is one with a more conservative approach and was developed through the use of a chemo-mechanical removal caries allied to the preservation of dental tissue.6
It propagates the use of prevention of extension and has gained popularity with technological improvements in tools for tooth preparation and with development of new adhesive systems.7
Chemo-mechanical caries removal (CMCR) agents were introduced in the 1970s and have the ability to dissolve softened tissue which can then be removed by manual excavation of carious dental tissues. The first CMCR material was introduced in 1975, called the GK 101, it was composed of a 5 % sodium hypochlorite (NaOCl) solution.8 Habib, Goldman, and Kronmann, observed that alone, a 5 % sodium hypochlorite solution could cause damage to tissues and hence launched Caridex which was 5 % sodium hypochlorite (NaOCl) in combination with sodium hydroxide, sodium chloride, and glycine.9 It did not show good results due to the need for large volume of solution, instability and complex equipment to be used, thus generating a high cost.
Towards the end of 1990s, a solution called Carisolv, was developed which contained 0.95 % sodium hypochlorite solution alongwith three amino acids (leucine, lysine, and glutamic acid).10 The reaction of NaOCl with amino acids led to degradation of collagen found in the demineralized portions of the carious lesion, thus neutralizing aggressive behavior in healthy tissues and allowing the rapid removal of caries. Its disadvantages were that it had a short shelf life, needed to be kept refrigerated, had a bad odor and required specially designed curettes for the removal of infected dentin, which increased the cost of the procedure.10
Papain, a protein extracted from papaya, containing gel was introduced in 2003 and was called Papacarie. It is easy to apply, does not require any elaborate equipment. Papain is responsible for dissolution of minerals from the exposed collagen in the dentin, softening the infected dentin further, which in turn aids in excavation using non-cutting instruments and without anaesthesia and rotary instruments.11
BRIX-3000, a papain-based chemicomechanical agent was introduced in 2012, alongwith a proteolytic enzyme which is collected from fruits of green papaya and leaves latex. This is available in gel form contained in a tube.11 It is bioencapsulated by EBE technology, which helps the gel to maintainan ideal pH tocontain the enzymes in inactivated form and deliver them when proteolysis of the collagen is required. Also it is known that there are no side effects of Brix3000, even if it is left in the cavity for longer because the enzyme will only work on the infected tissue and it will be inactive when it comes into contact with healthy tissue due to the presence of alpha-1 antitrypsin antiprotease.11
The objective of this study was to compare a chemical-mechanical removal of caries lesion using the enzymatic gel BRIX-3000 and the conventional method of caries removal, using No2/4 round burs.
METHODOLOGY:
A randomized controlled single-blinded clinical trial with forty samples. Keeping in mind the significance of power of this study a sample of 40 was selected for this study. Forty patients participated in the trial, and each was informed of the treatment procedure and a signed consent obtained from them. Forty permanent molars with Class 1 cavitated carious lesions were selected. Digital x-rays were utilized in standardizing the depth of caries in the selected teeth. The selection was based on the extent of the carious lesion and required caries to extend into the middle third of dentine.
Digital X-rays were taken for each tooth before selecting each sample into the trial. Once accepted into the trial, the samples were randomly divided into two groups, Group 1 where Brix3000, a chemomechanical agent was used to remove caries and Group 2 where conventional method, round bur No. 2/4 was used for caries removal.
Group 1 (n=20): The tooth to be treated was isolated with cotton rolls and saliva ejectors. BRIX3000 was applied to the cavitated lesion and left in the tooth for 2 minutes. A stopwatch was used to standardise the time. A spoon excavator was thereafter used to remove material along with infected dentin using a pendulum movement, without applying any pressure. BRIX3000 wasapplieduntil the gel after removing from the cavity looked similar to the gel contained in the syringe. The whole procedure was timed until the carious lesion was visually and tactilely determined to be removed (Figure 1).
Group 2 (n=20): The tooth to be treated was isolated with rubber dam. Caries was removed using conventional method with low speed round bur No 2/4. Burs used in each sample were new having the same ISO size and same operator performing caries excavation in all the cases. After the confirmation of complete removal of decayby the blinded investigators, the teeth were restoredwith glass ionomer cement and composite using sandwich technique.
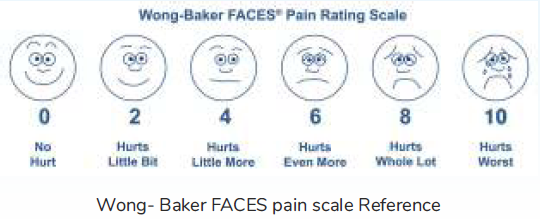
Wong-Baker FACES pain rating scale was used in this study to determine the level of pain after excavating caries with both the methods. The subjects chose the scale's face that best described how they felt throughout the procedure that they underwent. They were also enquired about the level of discomfort they felt and were asked to select one of three options: No discomfort or anxiety, mild discomfort or anxiety and Severe discomfort or anxiety. Alongwith this, a record of number of applications of BRIX3000 done per tooth, for the removal of carious lesion, was also maintained. The results were then compared and analysed.
RESULTS:
Forty young participants were enrolled in this study (20 Female and 20 Male) with a mean age of 26.45 ± 1.73(Table 1). Descriptive results of the time required for caries removal showed that on an average, BRIX3000 required 5.7minutesto remove all carious tissues which was longer than the time required by conventional rotary instrumentation method which was 3.1 minutes. Pairwise comparison using Mann-Whitney U test showed that the conventional rotary instrumentation method required significantly less time for caries removal as compared to Brix 3000, p=.001 (Table 2). The frequency and descriptive results, including the mean rank of the Wong-Baker scale for the evaluated groups, are reported. The Mann Whitney U test showed statistically higher pain score differences in the conventional rotary instrumentation method compared to Brix 3000, p=.002(table 3)Also, it was observed that higher discomfort was seen with conventional rotary instrumentation method compared to Brix 3000, although the difference was not statistically significant, p = .007(Table 4).
| GROUPS | SEX | MEAN AGE+_SD | RANGE | |
|---|---|---|---|---|
| MALES | FEMALES | |||
| BRIX3000 | 10 | 10 | 26.15 +- 2.121 | 22-30 |
| Conventional method | 10 | 10 | 26.15 +- 1.350 | 25-29 |
| TOTAL | 20 | 20 | 26.76 +- 5.810 | 16-35 |
| P value | 1.000 | .901 | ||
| GROUP | MEAN RANK | SUM OF RANK | p value | |
|---|---|---|---|---|
| Pain Grade | BRIX 3000 | 6.65 | 69.00 | |
| Conventional Bur | 14.35 | 141.00 | .002 |
| Group | ||||
|---|---|---|---|---|
| BRIX 3000 | Conventional | p value | ||
| Bur | ||||
| Discomfort | MD Count | 8 | 14 | .007 |
| ND Count | 12 | 0 | ||
| SD Count | 0 | 6 |
| GROUP | MINIMUM | MAXIMUM | MEAN TIME TAKEN +_ SD | P value |
|---|---|---|---|---|
| BRIX3000 | 5.0 | 7.0 | 5.750+-.8250 | .001 |
| Conventional method | 1.0 | 5.0 | 3.1+-1.3703 |
DISCUSSION:
Minimally Invasive Dentistry (MID) is a concept of maximum preservance of the healthy tooth structure during dental treatment. For success, the dental surgeon must be aware of the difference between conservation and elimination of tooth structure. MID isa conservative approach.12 However, the most commonly used technique to remove caries is through the conventional methods: use of rotary hand piece with low-speed burs.
A lot of reluctance is seen among patients seekingh dental treatment due to the pain and/or discomfort caused due to conventional cavity preparation methods. Besides, the frequent need for local anaesthesia, to control the pain caused with rotary instruments during caries removal in deep carious lesions, is a potential factor for discomfort and pain.13 Rotary instruments are the greatest triggers for fear and anxiety, which are two most common reasons for avoidance or postponement of dental treatment.
Rotary instrumentation has many disadvantages, as it is comparatively more invasive, the sound and feel of rotary instrumentation is much to the patient's dislike, and it could be potentially harmful to pulpal tissue due to excessive cutting.13 Vibration, sound, and discomfort induced by mechanical method of caries removalhave shown to have an overall unpleasant treatment experience and were, the triggers for a more uncooperative behaviour during treatment.14 On the other hand, alternative methods such as CMCR agents has shown toresult in higher acceptance and a more comfortable treatment experience.
Chemomechanical methods provide a good line of treatment for more conservative removal of caries.14 There have been several recent studies concentrating on chemo-mechanical caries removal agents (CMCR) as an MID method for excavating carious dental tissues.16,17,18 In the present study, comparison between a CMCR agent (Brix 3000) and a conventional rotary instrumentation methods was carried out for the acceptance of the technique and the time required to remove caries in subjects enrolled in the study. Each patient enrolled in the present study was evaluated after excavating the caries. Tactile assessment was done to assess the effectiveness of caries removal in this study. Visual and tactile detection of caries is a verified method according to many systematic reviews and studies.
Methods of caries detection, such as caries detection dyes may cause unnecessary removal of sound tooth structure, as they can stain the organic matrix of less mineralized dentin, including sound dentin at dentin-enamel junction (DEJ).16 In a study by Sadasiva et al., the tactile method of detecting caries was found to be as efficient as caries dye or laser fluorescence in evaluating remaining dentinal caries.17,18 In another study by Banerjee et al., it was reported that the use of dyes is not recommended in lesions which extend upto the middle third of dentin or deeper, due to the inadvertent risk of over cutting which might often result in pulpal involvement which could have been avoided otherwise.19 Therefore, the tactile method of detection is considered to be more conservative than others as one of the most important aims of using CMCR in dentistry is to conserve as much dental tissues as possible.15
Furthermore, many factors can affect the results in the excavation of caries such as the operator, the excavator and softness of carious dentin.20,22 So, in order to have a standardized protocol, a single practitioner performed excavation of caries for all teeth with the same type of hand excavator.
Face scales are being used predominantly for pain measurement since the 1980s.21 Many studies have evaluated different scales to assess the validity and reproducibility of the scale that makes it applicable in researches. Wong-Baker FACES pain rating scale is composed of six faces of pain rated 0-10, in which the subject is instructed to point to the face that represents his/her level of discomfort during treatment. Two blinded examiners helped in deciding the health of remaining dentin within each cavity.
Chemo-mechanical caries removal was significantly slower compared to the conventional method. This finding was consistent with the invitro study done by Kitsahawong et al., which showed that the meantime for caries removal using Papacarie was significantly higher than the conventional method.23 The mean pain score, obtained by this study, was significantly higher with the use of conventional method as compared to CMCR. These findings are in accordance and comparable with Singh et al., who demonstrated less pain sensation than conventional methods using Papacarie which has a mode of action that involves the removal of dead infected dentin through the degradation of proteoglycan matrix.24 Kleinknecht et al. reported that dental anxiety mainly results from invasive dental procedures such as "injections" and "drilling", while these are not needed with the use of CMCR agents.25
Limitations of this study are the dependence on manual detection of caries only and the small sample size. Also, since the same operator excavated in all cases, there could be an operator bias. So, further studies are required to check the overall efficiency of the material.
CONCLUSION:
Within the limitations of this study, it was concluded that BRIX3000 is an efficient replacement to conventional caries removal method despite of its longer working time. Although it cannot completely replace the conventional drilling method, it seems to be a promising CMCR agent having lower pain score and discomfort compared to conventional drilling method. However, further studies should be conducted to clarify the real scope of BRIX3000 in clinical practice.
REFERENCES:
- Dental caries and their association with socioeconomic characteristics, oral hygiene practices and eating habits among preschool children in Abu Dhabi, United Arab Emirates - the NOPLAS project. BMC Oral Health. 2018;18:104.
- [CrossRef] [PubMed] [Google Scholar]
- Caries pathology and management in deep stages of lesion formation. In: Bjørndal L, Kirkevang L-L, Whitworth J, eds. Textbook of Endodontology (3). Oxford; UK: Wiley Blackwell; 2018. p. :61-78.
- [CrossRef] [Google Scholar]
- The International Caries Detection and Assessment System (ICDAS): an integrated system for measuring dental caries. 2007. Community Dent Oral Epidemiol. 35:170-178.
- [CrossRef] [PubMed] [Google Scholar]
- Grossman's endodontic practice. (13th). Lipincott: Williams and Wilkins; 2010. p. :310-330.
- [Google Scholar]
- Comparison of anxiety levels associated with noise in the dental clinic among children of age group 6-15 years. 2013. Noise & health. 15:190-193.
- [CrossRef] [PubMed] [Google Scholar]
- Minimally Invasive Dentistry: A Conservative Approach to Smile Makeover. CompendContinEduc Dent (Jamesburg, N.J. : 1995). 2017;38(1):38-42. PMID: 28054792
- [Google Scholar]
- Extension for prevention: is it relevant today? Am. J. Dent. 1998;11(4):189-196. PMID: 10388375
- [Google Scholar]
- Chemomechanical caries removal in primary teeth in a group of anxious children. 2003. J. Oral Rehabil. 30:773-779.
- [CrossRef] [PubMed] [Google Scholar]
- Chemo-mechanical method: a valuable alternative for caries removal. J Minim Interv Dent. 2009;2(4):248-260.
- [Google Scholar]
- A Review on Agents for Chemomechanical Caries Removal. Sch J Dent Sci J Dent Sci. 2016;3(9):264-268.
- [CrossRef] [Google Scholar]
- Chemomechanical caries removal: a comprehensive review of the literature. 2001. Int Dent J. 51:291-299.
- [CrossRef] [PubMed] [Google Scholar]
- Minimal intervention dentistry - a new frontier in clinical dentistry. 2014. J ClinDiagn Res. 8:ZE04-ZE8.
- [CrossRef] [PubMed] [Google Scholar]
- Weefselbesparendetandheelkunde. Eenrevolutionair concept? [Minimal invasive dentistry. A revolutionary concept?] Ned Tijdschr Tandheelkd. 2003;110(6):215-217. PMID : 12852055
- [Google Scholar]
- Chemomechanical caries removal: a comprehensive review of the literature. 2001. Int Dent J. 51:291-299.
- [CrossRef] [Google Scholar]
- Treatment of caries in relation to lesion severity: implications for minimum intervention dentistry. 2015. J Dent. 43:58-65.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy of chemomechanical caries removal in reducing cariogenic microbiota: a randomized clinical trial. 2014. Braz Oral Res. 28 S1806 - 83242014000100242
- [CrossRef] [PubMed] [Google Scholar]
- A comparative study of the clinical efficiency of chemomechanical caries removal using Carie-Care gel for permanent teeth of children of age group of 12-15 years with that of conventional drilling method: A randomized controlled trial. Dent Res J (Isfahan). 2019;16(1):42-46. PMID: 30745918
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of the Efficacy of Visual, Tactile Method, Caries Detector Dye, and Laser Fluorescence in Removal of Dental Caries and Confirmation by Culture and Polymerase Chain Reaction: An In Vivo Study. 2019. J Pharm Bioallied Sci. 11:S146-S150.
- [CrossRef] [PubMed] [Google Scholar]
- In vitro validation of carious dentin removed using different excavation criteria. Am J Dent. 2003;16(4):228-230. PMID: 14579874
- [Google Scholar]
- Pain in children: comparison of assessment scales. Pediatr Nurs. 1988;14(1):9-17. PMID: 3344163
- [Google Scholar]
- Instruments and equipments. In: Gopikrishna V., ed. Preclinical Manual of Conservative Dentistry. Elsevier, India; 2011. p. :37-104.
- [Google Scholar]
- Evaluation of nanoleakage following deproteinization of dentin using varying concentrations and application times of sodium hypochlorite solution and gel-an in vitro confocal laser scanning microscope study. J Conserv. Dent. 2005;8(1):27.
- [CrossRef] [Google Scholar]
- Comparative clinical evaluation of chemomechanical caries removal agent Papacarie® with conventional method among rural population in India-in vivo study, Braz. J. Oral Sci. 2011;10(3):193-198.
- [Google Scholar]
- Behavioral changes in preschoolers treated with/without rotary instruments. J IntSocPrev Community Dent. 2014;4(2):77-81.
- [CrossRef] [PubMed] [Google Scholar]
- Behavioral changes in preschoolers treated with/without rotary instruments. J IntSocPrev Community Dent. 2014;4(2):77-81.
- [CrossRef] [Google Scholar]




